Her problems began about four years after the gastric bypass surgery. Doctors at Vanderbilt University Medical Center were too stupid and too lazy to figure out what was killing her. No nutritional equation worked because her body was turning protein into ammonia and her liver was failing to convert it to urea. Her body could not excrete the toxin.
Cynthia Le Mons, executive director of the
National Urea Cycle Disorders Foundation, believes the complication that
led to Hilary X's death is not as rare as doctors think. She knows
of six women who have developed urea cycle failure after gastric bypass
surgery since 2007. Five of the six died.
"That's just the tip of the iceberg," Le Mons said. "If we know about it, it's just a microcosm of what is going on."
Read more about how greedy butcher doctors killed Hilary Lane.
 |
| A Biologist or an Engineer Can Understand This Most Doctors Can't! Doctor's Are Not All That Bright |
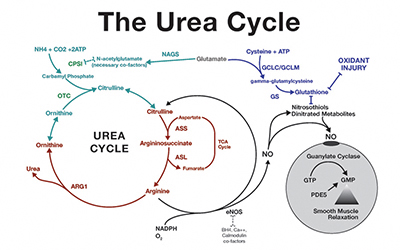
L-citrulline is a non-essential amino acid. In hepatocytes, the addition of carbon dioxide and ammonia to ornithine synthesizes L-citrulline during the urea cycle. The enzymes argininosuccinate synthetase and argininosuccinate lyase, when in the presence of L-aspartate and ATP, converts L-citrulline into L-arginine . Subsequently, L-arginine is converted to nitric oxide by nitric oxide synthase and L-citrulline is regenerated as a by-product .
Citrulline, a non-standard amino acid not normally present in protein, is an intermediate in the conversion of the amino acid ornithine to arginine during the urea cycle.
Citrulline Uses
Citrulline’s main function is its ability to remove ammonia and is essential for the excretion of oxidative waste processes. It is also used for treatment of Ornithine Transcarbamylase, a urea cycle disorder. Urea cycle disorder is a genetic disorder consisting of a deficiency of one of the enzymes needed in the urea cycle. Citrulline is critical in the improvement of immune system deficiencies and overall functioning.
Malic Acid, a key component of the energy production yielded via the Kreb’s cycle, conditions and assists lactate and pyruvate toward anabolism rather than catabolism. Supplementation of this nonessential amino acid has reduced fatigue significantly as well as increase energy production. Documentation has shown citrulline to significantly increase the body’s metabolic rate, aerobic performance, and provide reductions in the onset of muscular fatigue.
In conclusion, citrulline supplementation may not only boost physical activity performance, but also provide our bodies with a means of eliminating the amino acid breakdown products of protein metabolism. Equally important is the detoxification of ammonium and lactate from the blood.